
|
As the standards of ethical behavior and regulations have been amended and expanded, contemporary health care is a prerequisite for sound decision-making and planning and an essential step in the development of rational public policy for health.To ensure and maintain that the highest levels of ethical standards in the field of health informatics are carried out, this will ultimately rely on the ability of the health informaticist to exercise judgment in identifying and assessing differences in values (Prosperi et al., 2018).
Load More
In this connection, it is essential to note that codes of professional ethics fundamentally differ from obligations beyond what the law requires (Kluge, 2011). Legal provisions provide the ideology of professional regulation within which a profession focuses on diversity and conflict of interest and their implications for change. Moreover, statutory provisions are formulated by legislators, judges, or juries regarding current and anticipated circumstances having legal consequences as these are understood as the interaction of a unitary State and a homogeneous community. Therefore, according to Muthuchidambaram (1988), statutory provisions and legal codes are time-bound and can provide little guidance when unexpected technical developments occur. Shaping the profession of Health Informatics, here are some implications of ethical, legal, and social issues for personal health and applications:
|
According to O’Carroll (2003), “one of the most critical current laws affecting health informatics is the Privacy Act of 1974.”This law requires 1) that federal agencies provide public notice of their records systems by publishing them in the Federal Register and 2) written consent from subjects before a record can be released and provided a process by which questions can access or change their records.
Initially limited to sharing health and patient records and confined to national pockets, managed by individual National Health Systems (NHS) (Leiyu & Singh, 2004), eHealth services have since expanded to secure methodologies for achieving international interoperability, in turn, is problematic for Health Informaticists. Load More
For instance, when the eHealth providers store their EHRs in jurisdictions other than those where the service is delivered, the privacy rights of patients in the jurisdiction-of-delivery may be different from those of the jurisdiction-of-storage, and what is recognition of universal civil jurisdiction and can the latter be limited to Congressional Power under the former (Edmunds, 2014; Szerejko, 2014)?
According to Tribbensee (2003), when the eHealth care providers or organizations that provide informatic services to health care providers that are incorporated in jurisdictions like the USA, where provisions like the USA PATRIOT Act (McCarthy, 2002) or legal regulations like it are in force, such providers or organizations and by extension, their subsidiaries may be required to produce or provide access to any EHR that they hold with ethical justification for conducting public health surveillance without patient knowledge or consent. Reference
Edmunds, M. (2014). Governmental and legislative context of informatics. In Public health informatics and information systems (pp. 47-66). Springer, London. Hübner, U., Shaw, T., Thye, J., Egbert, N., de Fatima Marin, H., Chang, P., ... & Ball, M. J. (2018). Technology informatics guiding education reform–TIGER. Methods of information in medicine, 57(S 01), e30-e42. Hovenga, E. J., Kidd, M. R., & Garde, S. (Eds.). (2010). Health informatics: an overview (Vol. 151). Ios Press. Keshta, I., & Odeh, A. (2021). Security and privacy of electronic health records: Concerns and challenges. Egyptian Informatics Journal, 22(2), 177-183. Kluge, E. H. W. (2011). Ethical and legal challenges for health telematics in a global world: telehealth and the technological imperative. International journal of medical informatics, 80(2), e1-e5. Leiyu, S., & Singh, D. A. (2004). Delivering health care in America: a system approach. Lehne, M., Sass, J., Essenwanger, A., Schepers, J., & Thun, S. (2019). Why digital medicine depends on interoperability. NPJ digital medicine, 2(1), 1-5. Magrabi, F., Ong, M. S., Runciman, W., & Coiera, E. (2012). Using FDA reports to inform a classification for health information technology safety problems. Journal of the American Medical Informatics Association, 19(1), 45-53. Muthuchidambaram, S. (1988). Information technology, citizens’ rights, and personnel administration. In Technology and Contemporary Life (pp. 193-215). Springer, Dordrecht. National Research Council (U.S.). (1997). For the record: Protecting electronic health information. Washington, D.C: National Academy Press. O'Carroll, P. W. (2003). Public health informatics and information systems. New York: Springer. Prosperi, M., Min, J. S., Bian, J., & Modave, F. (2018). Big data hurdles in precision medicine and precision public health. BMC medical informatics and decision making, 18(1), 1-15. Ratwani, R. M., Reider, J., & Singh, H. (2019). A decade of health information technology usability challenges and the path forward. Jama, 321(8), 743-744. Singh, H., & Sittig, D. F. (2016). Measuring and improving patient safety through health information technology: The Health IT Safety Framework. BMJ quality & safety, 25(4), 226-232. Subbian, V., Solomonides, A., Clarkson, M., Rahimzadeh, V. N., Petersen, C., Schreiber, R., ... & Senathirajah, Y. (2021). Ethics and informatics in the age of COVID-19: challenges and recommendations for public health organization and public policy. Journal of the American Medical Informatics Association, 28(1), 184-189. Szerejko, J. D. (2014). Reading between the lines of electronic health records: the health information technology for economic and clinical health act and its implications for health care fraud and information security. Conn. L. Rev., 47, 1103. Torous, J., Nicholas, J., Larsen, M. E., Firth, J., & Christensen, H. (2018). Clinical review of user engagement with mental health smartphone apps: evidence, theory and improvements. Evidence-based mental health, 21(3), 116-119. Tribbensee, N. (2003). Privacy and security in higher education computing environments after the USA PATRIOT Act. JC & UL, 30, 337 |

|

|
Health burdens are sustained and magnified by rhetoric along with immigration policies and laws that increase fear of detection, language barriers, and lack of knowledge about the health care system, all of which limit the ability to effectively access health services and impact health outcomes, including mental health.Healthcare professionals, politicians, stakeholders, think tanks, advocacy groups, and others should come together and respond with policy solutions based on social justice and human rights premises.
As Rebecca Onie stated (2018), "How do you create a healthcare system without asking the person if they are hungry? Also, healthcare professionals and providers should develop strategies to eliminate discrimination in healthcare settings by developing and implementing more inclusive policies. Load More
While many of these policies might interfere with the provider's right to provide services to specific groups, health providers should respond to the humanitarian call embedded in the profession that entails providing health care for all. We all know the things we need to get healthy, but these are not what we need to be healthy (Onie, 2018, as cited in Gordon,2019). The purpose of health insurance is to increase services associated with care coordination and provide protection against high out-of-pocket costs. Health outcomes are determined by the genetic, environmental, process, and social supports as buffers of life, and evidence that Medicaid or any other type of health coverage improves not just access to care but is restricted depending on the environment with which health care is provided. Medicaid beneficiaries access health care at rates comparable to the standards for privately insured people and sharply higher rates than the uninsured. By making healthcare affordable, Medicaid increases economic security for low-income households. However, how does living paycheck to paycheck affect your mental wellbeing? How many of us have at least 3-months of necessary living expenses saved up for an emergency? How many of us are prepared for a catastrophic medical event, and how much will your out-of-pocket be? |
Technological advances in medical science have allowed health care providers to diagnose and treat illnesses in previously impossible ways.In general, such developments have tended to increase healthcare spending, which has been seen as an essential policy concern, especially considering ever-limited healthcare budgets.
However, examining the link between the knowledge base concerning the financing of healthcare and health outcomes is only one part of the picture. To better understand the dynamics between the intangibles, innovation, and spending, it is critical to assess whether and under what circumstances result in better value in health care. Load More
Are we attaining weight from the technologies developed, and for what cost? Out-of-pocket payments, individual private insurance, employment-based private insurance, and government financing are the modes of healthcare financing impacting healthcare development and implementation. For example, I can still retain my health insurance if I were unemployed. I may qualify for health insurance through the Consolidated Omnibus Budget Reconciliation Act (COBRA) (Lynch, 2018). If I had preexisting conditions, this might be the most cost-effective option. But as a somewhat healthy individual, this option is not realistic. However, the State of California requires residents to maintain health insurance or be subject to a tax penalty. In comparison to my wife's health benefits package, which includes herself and our three children, she has a low copay ($20-$35), deductible ($500), and a monthly installment of $100. I have a monthly payment of $262 with a high copay and deductible for myself alone. Again, if I were unemployed, would it still be less expensive to "pay as I go" and pay the penalty at the end of the year? Reference
Gordon, M. (2019). Becoming a Social Entrepreneur: Starting Out, Scaling Up and Staying True. United Kingdom: Taylor & Francis. Lynch, M. S. (2018). Budget Reconciliation Measures Enacted Into Law: 1980- 2017. Congressional Research Service. Onie, R. (2018). Why Don't We Deliver the Health We Should?. NEJM Catalyst, 4(2). |

|
Policy Position: Healthcare Affiliation Among Physician Organizations

|
The US government has created a combination of enforced legislation and financial incentives for healthcare organizations and eligible professionals to use electronic health record (EHR) systems that will meet the Centers for Medicare & Medicaid Services (CMS) statutory criteria of meaningful use while simultaneously helping providers improve (William, 2017).At the same time, according to Gold & McLaughin (2016), providers that have merged or formed integrated delivery systems of EHRs indicate a variety of pitfalls associated with health IT adoption, including (Eickholt, 2019) lack of hardware, infrastructures, strategic planning in the field of electronic health records, and physicians and clinical staff's resistance.
Load More
Administered by the Office of the National Coordinator (ONC) for Health Information Technology (HIT) (Davey et al., 2022), the Regional Extension Center (REC) is a federally funded program that is dedicated to and supporting the adoption of health information technology and the promotion of a nationwide health information system exchange to improve healthcare.
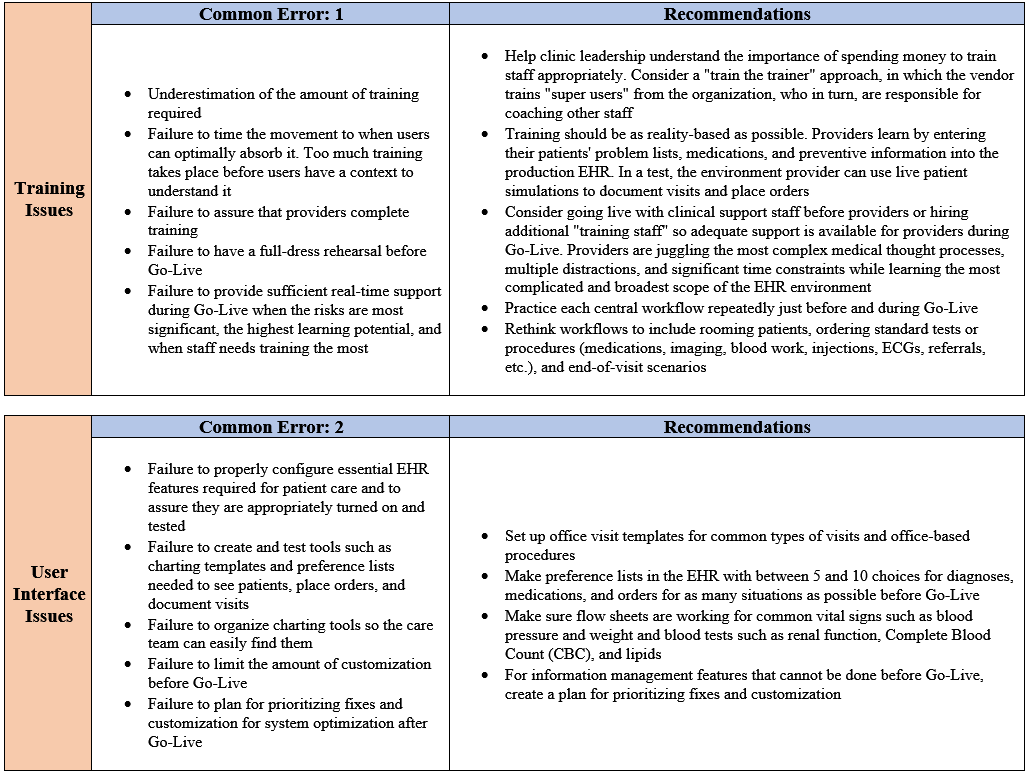
Pozgar (2020) states this includes outreach and education, EHR vendor support, workflow redesign assistance, and change management support. Through the passage of the American Recovery and Reinvestment Act of 2009, according to the Senate et al. (2018), the ONC has funded more than 62 RECs and 100,000 primary care providers to adopt the use of EHRs. In this illustrative embodiment, each error carries associated costs that reduce the likelihood of successful adoption, seriously jeopardize a medical practice's financial viability, and negatively impact patient care. |
Facilitated with one or more exemplary data structures, I present a Business Intelligence (BI) solution for two common errors in EHR Implementation contributing to practice disruption.
Reference
Davey, K. S., Johnson, J. A., Greenhill, R. G. (2022). Sultz and Young's Health Care USA: Understanding Its Organization and Delivery. (n.p.): Jones & Bartlett Learning.
Eickholt, L. (2019). Why many integrated delivery systems have not enhanced consumer value, and what's next. NEJM Catalyst Innovations in Care Delivery, 1(1).
Gold, M., & McLaughlin, C. (2016). Assessing HITECH implementation and lessons: 5 years later. The Milbank Quarterly, 94(3), 654-687.
Pozgar, G. D. (2020). Legal and ethical essentials of health care administration. Jones & Bartlett Learning.
Senate, U. S., Resources, Committee on Energy and Natural. (2018). American Recovery and Reinvestment Act of 2009. (n.p.): CreateSpace Independent Publishing Platform.
Williams, J. (2017). The CMS Innovation Center's expansion authority and the logic of payment reform through rulemaking. Journal of Health and Human Services Administration, 3-43.
Eickholt, L. (2019). Why many integrated delivery systems have not enhanced consumer value, and what's next. NEJM Catalyst Innovations in Care Delivery, 1(1).
Gold, M., & McLaughlin, C. (2016). Assessing HITECH implementation and lessons: 5 years later. The Milbank Quarterly, 94(3), 654-687.
Pozgar, G. D. (2020). Legal and ethical essentials of health care administration. Jones & Bartlett Learning.
Senate, U. S., Resources, Committee on Energy and Natural. (2018). American Recovery and Reinvestment Act of 2009. (n.p.): CreateSpace Independent Publishing Platform.
Williams, J. (2017). The CMS Innovation Center's expansion authority and the logic of payment reform through rulemaking. Journal of Health and Human Services Administration, 3-43.
EPIC EHR Implementation Project
|
The Standards for Privacy of Individually Identifiable Health Information (Privacy Rule) establishes end-to-end, health-based systems and methods to achieve the Health Insurance Portability and Accountability Act of 1996 (HIPAA) (Gaylor, 2012) as specified by the U.S.Department of Health and Human Services (HHS) according to (Hersh & Hoyt, 2018).
Addressing the disclosure practices, development of reporting standards, and asymmetry of identifiable information (Liu et al., 2015), the Office for Civil Rights (OCR), whether obtained by independent or proceeding with another action (Debra, 2012), has the responsibility to vindicate agency enforcement policy or to compel compliance with the terms of the orders, including relief that a court would lack the power to provide (Field, 2007; Journal of the House of Representatives of the United States, 1813). Load More
Ensuring health coverage, equitable treatment, high-quality health care, and consumer choice at an affordable cost, the Privacy Rule complies with an optimized approach that permits enterprise-wide data integration and analysis while preserving the ethics of those seeking a spiritual dimension of care development toward healing. |
HIPAA compliance is not the only ethical challenge in managing health information. Since the implementation of HIPAA, Electronic Health Records (EHRs), and Health Information Exchange (HIE), the industry has been riddled with paper and electronic health information breaches and identity theft on an ongoing basis.
Between 2009 and 2019, the HIPPA Journal (2020) reported 3,054 data breaches that involved 500 records. Within those records, at a rate of 1.4 violations per day, 230,954,151 million pieces of information equate to almost 70 percent of the U.S. population.
Except for additional enforcement information, the security and privacy rules have not been amended, which has led to Public Health Records being promoted and developed to include (Quigley, 2008):
Except for additional enforcement information, the security and privacy rules have not been amended, which has led to Public Health Records being promoted and developed to include (Quigley, 2008):
- Those offered by HIPAA-covered entities
- Self-contained products operated by the consumer
- PHRs operated by a third party with data provided by the consumer
- Health record banks, where an entity stores information from a variety of entities related to the consumer and where disclosure is only at the direction of the consumer
Load More
To protect patient data without sacrificing the usability and accessibility of the information, healthcare organizations should have a defined patient development response to minimize the chance of maximum consequence.
Patient data storage, network security, and digital communications are just a few ways that technology functions in the day-to-day operations of medical practice. As pressure rises, Congress must address health information privacy, especially in an electronic information world.
Likely manifest, there is no one hundred percent agreement on what constitutes privacy of healthcare data or how privacy should be addressed in the current environment of new technology to improve aggregate reports that combine clinical and administrate data.
Created at state and federal levels to protect registries for evaluating patient outcomes, this is becoming increasingly important as groups strive to develop clinical information systems to facilitate patient management, support, and feedback in patient teaching.
Patient data storage, network security, and digital communications are just a few ways that technology functions in the day-to-day operations of medical practice. As pressure rises, Congress must address health information privacy, especially in an electronic information world.
Likely manifest, there is no one hundred percent agreement on what constitutes privacy of healthcare data or how privacy should be addressed in the current environment of new technology to improve aggregate reports that combine clinical and administrate data.
Created at state and federal levels to protect registries for evaluating patient outcomes, this is becoming increasingly important as groups strive to develop clinical information systems to facilitate patient management, support, and feedback in patient teaching.
References
Debra Cascardo, M. A. (2012). Part I is what to do before the Office for Civil Rights comes knocking. The Journal of Medical Practice Management: MPM, 27(6), 337.
Field, R. I. (2007). Health care regulation in America: Complexity, confrontation, and compromise.
Gaylor, L. J. (2012). The Administrative Dental Assistant. United Kingdom: Elsevier - Health Sciences Division.
Hersh, W. R., & Hoyt, R. E. (2018). Health Informatics: Practical Guide Seventh Edition. Lulu.com.
Journal of the House of Representatives of the United States. (1813). United States: Francis Childs and John Swain.
Liu, V., Musen, M. A., & Chou, T. (2015). Data breaches of protected health information in the United States. Jama, 313(14), 1471-1473.
Quigley, M. (2008). Encyclopedia of information ethics and security. Hershey: Information Science Reference.
Field, R. I. (2007). Health care regulation in America: Complexity, confrontation, and compromise.
Gaylor, L. J. (2012). The Administrative Dental Assistant. United Kingdom: Elsevier - Health Sciences Division.
Hersh, W. R., & Hoyt, R. E. (2018). Health Informatics: Practical Guide Seventh Edition. Lulu.com.
Journal of the House of Representatives of the United States. (1813). United States: Francis Childs and John Swain.
Liu, V., Musen, M. A., & Chou, T. (2015). Data breaches of protected health information in the United States. Jama, 313(14), 1471-1473.
Quigley, M. (2008). Encyclopedia of information ethics and security. Hershey: Information Science Reference.